We’re back (after a brief hiatus) with an update on Fukushima radiation and seafood, and answers to several of your questions.
In this episode, we cover:
2:41 Is There Really Fukushima Radiation in My Fish?
14:16 The truth about “eating too much meat”
18:50 Naturally healing cavities
23:50 Hepatitis C and Liver Disease
30:03 What to do about esophagitis and GERD
33:27 Is resistant starch useful?
37:18 Treating skin conditions with FMT
Full Text Transcript:
Steve Wright: Hey, everyone. Welcome to another episode of the Revolution Health Radio Show. This show is brought to you by ChrisKresser.com, and I’m your host, Steve Wright from SCDLifestyle.com. With me is integrative medical practitioner and healthy skeptic Chris Kresser. So, Chris, how’s your day going?
Chris Kresser: It’s pretty good, Steve. How are you?
Steve Wright: Mine is going very well as well.
Chris Kresser: Great.
Steve Wright: It’s just been a busy day.
Chris Kresser: Yeah. So, I’m sure folks have noticed that it’s been a while since we did a podcast. We’ve been pretty regular about it the past few years, but life intervened and I’ve been so overwhelmingly busy with the book and putting the final touches on that, finishing the manuscript, responding to the copyedits and getting that ready, and then doing some media stuff related to it that I just couldn’t find the time to do a podcast, so here we are! Know that I can’t guarantee an every-other-week, regular show between now and maybe February or March because of all the book activities, but I’ll do my absolute best to keep the show going during that time. And we’re going to have lots of other great stuff for you, too, in the next few months related to the book, so hopefully you won’t miss it too much if we miss a week or two here and there.
Steve Wright: Yeah, we appreciate everyone’s patience with Chris’ schedule and know that Chris puts a lot of time and effort into these podcasts. I just talk, so it’s not a huge burden for me, but Chris works his butt off to get ready for these types of podcasts. So, Chris, we’re going to start with a little talk of Fukushima, and then we’re going to transition over to some long-awaited Q&A.
Chris Kresser: Sounds great.
Steve Wright: All right. Well, before we get into radioactive substances in seafood, let me tell you all about Beyond Paleo. If you haven’t heard yet, Chris put together his best tips and tricks into a free 13-part email series that well over 30,000 people have already downloaded and basically subscribed to. It’s an email series. It’s going to blast you an email every so often, again, with Chris’ best tips and tricks on burning fat, boosting energy, and preventing and reversing disease without drugs. So, it’s pretty simple. If you’d like this and you don’t have this info yet, you just go over to ChrisKresser.com, look for the big red box, and go ahead and put your name and email in that box, and Chris will start sending you those free emails.
Is There Really Fukushima Radiation in My Fish?
So, Chris, there’s been a lot of talk about radioactive substances in the water and seafood. What’s going on here?
Chris Kresser: Yeah, so I’ve heard from a lot of people, both in my personal life, family members, friends, and then also on the blog, podcast questions, just people I meet here and there – everyone wants to know if they should be wary of eating seafood because of the Fukushima radiation. And there has been a lot of fear-mongering type of articles on the Internet, sites like Natural Health News and other similar types of sites that claim that the levels of radiation in fish are harmful and we should be taking all kinds of detox supplements to try to get rid of this excess radiation and we should be avoiding any fish that’s caught in the Pacific Ocean. As usual, we always want to look at all these kinds of claims with a grain of skepticism and look to the scientific literature to see if these claims can actually be substantiated by peer-reviewed evidence, and this is especially true when you’re talking about stopping consumption of a type of food that most people don’t get enough of and that’s extremely nutrient dense, that contains long-chain omega-3 fats that are really impossible to get anywhere else in the diet in their preformed state and one of the sole sources of vitamin D in the diet as well. And if there’s anything most people need to be concerned with, it’s not eating enough fish rather than eating too much of it. So, whenever there’s some kind of claim that we shouldn’t be eating fish, it has to, of course, be evaluated very seriously because there are actual health repercussions for not eating fish. I mean, if there was a claim that we shouldn’t eat industrial seed oil or… I don’t know… eggplants? If something happened to them where they became toxic and we couldn’t eat eggplants anymore, I think we could get by. We’d still want to evaluate that claim because there’s no sense in removing a food like that from our diet if we don’t have to, but the seriousness of it isn’t at the level of telling someone to remove fish because we’ve spent so much time studying the health benefits of the nutrients that fish contain, and I think that it’s really, like I said, important that people continue to eat it if that makes sense.
It’s completely natural and appropriate to be concerned about radiation, and I think there’s also a little bit of hysteria around radiation that makes sense on a certain level as well. It’s kind of a scary thing. You can’t see it. It’s potentially fatal, life threatening, it’s a way of getting sick and then perhaps dying that seems particularly egregious. And for whatever reason, there’s just a very heightened level of concern about radiation for better or for worse. And there is obviously a real issue here with Fukushima radiation. In fact, some recent news reports suggest that the radiation is not only still occurring, but it’s actually possibly occurring at a greater rate than ever. Steve actually just sent me a couple articles today about that. So, this is a significant concern. But the question that we’re talking about today is whether eating seafood that has been contaminated with radioactive isotopes from the Fukushima fallout will cause health problems. That’s the only question that we’re talking about today. And hopefully you’ll be relieved to know that all the peer-reviewed studies that have looked at this question have found that there’s not even a miniscule risk of getting sick from eating fish caught in the Pacific.
There was one large review in the Proceedings of the National Academy of Sciences, PNAS, the journal, and it evaluated the health risk of consuming Pacific Bluefin tuna that was caught in the Pacific after the Fukushima event around San Diego, I believe is where the fish were caught were for this study. And the study was done by some researchers from the Woods Hole Oceanographic Institution and a couple other organizations around the world, and they’re all independent researchers. There were no conflicts of interest, nobody that was working for the fish lobby! And let me just highlight a few of the findings for you. They estimated that a typical restaurant-sized portion of Pacific Bluefin tuna that was contaminated with radioactive isotopes cesium-134 and cesium-137 contains about 5% of the radiation you’d get from eating one uncontaminated banana and absorbing its naturally occurring radiation.
The really important thing to remember here is that all foods contain radiation because there’s radiation that’s just naturally a part of our planet. Bananas contain much more radiation in them, despite not being contaminated by Fukushima fallout, than a restaurant-sized portion, a 7-ounce portion, of fish. So, the issue is not whether we’re exposed to radiation, because we are, all of us, on a daily basis exposed to radiation in food, just walking around. If we go on a cross-country flight, we’re exposed to radiation. Like every other toxin, the question is what’s the dose? A small amount of toxin we can handle. A large amount of toxin causes problems. That’s really important to keep in mind with this. It is true that cesium-134 and cesium-137, which are these radioactive isotopes, have been found in fish because of Fukushima, but the levels are so low that they’re not going to cause any health problems, even in people who are eating fish at extremely high levels. For example, if you ate three-quarters of a pound a day of this contaminated Bluefin tuna for an entire year, you’d still receive only 12% of the dose of radiation you’re exposed to during a single cross-country flight from LA to New York. That should put it into perspective a little bit. Also, at that same level of consumption, the excess relative risk of fatal cancers would only be two additional cases per 10 million similarly exposed people, and that’s such a low number that in statistics and health there’s really reason to believe that’s no more than chance. And, in fact, statistically significant elevations in cancer risk are only observed typically at doses of radiation that are 25,000 times higher than what you’d expect to be exposed to by eating the three-quarters of a pound a day of Bluefin tuna.
The other thing – and I mentioned this before with the banana example – is that levels of naturally occurring radioactive isotopes, like polonium-210 and potassium-40, in Bluefin tuna are greater by several orders of magnitude than the radioactive isotopes from the Fukushima contamination in the fish, which is cesium-134 and cesium-137. In fact, levels of polonium-210 in fish prior to the Fukushima event were 600 times higher than the levels of cesium from Fukushima that were found. This suggests that the additional radiation in the form of cesium from Fukushima is completely insignificant from a health perspective.
Another thing I want to mention is that there are some bottom-feeding fish that are right off of where the reactor is in Japan, right off the coast, that contain extremely high levels of radiation, like 250 times more cesium in those fish or more than what are found in Pacific Bluefin tuna, and even if you consumed a third of a pound per day of this really highly contaminated fish, you’d still be below the international dose limit for radiation exposure from seafood.
And then the last thing that I want to point out is that Dr. Robert Emery at the University of Texas Health Center in one article said that you’d need to eat 2-1/2 to 4 tons of tuna in a year to get a dose of cesium-137 that exceeds the recommended health limit. So, to put that in perspective, that’s 14 to 22 pounds of tuna a day that you would have to eat to have a problem from this radiation in fish. All of that to say at least right now I have not seen any peer-reviewed, reliable evidence to suggest that there’s any problem eating seafood caught in the Pacific. Of course, I’ll continue to evaluate this, and if anyone has seen any studies published in a reputable journal that contradict this, I would be happy to look at them, and I’ll be the first person to change my mind if I see such evidence. But like I said before, articles on Internet sites that aren’t substantiated and don’t contain references to peer-reviewed research, you really can’t rely on those. I don’t see any evidence of a conspiracy within the scientific community to cover this up. Scientists that work at oceanographic institutes and other independent organizations don’t really have any reason to cover this up. There’s no plausible motivation for it. So, that’s my current take on it.
Steve Wright: Yeah, thanks, everyone, for listening to this episode of myth-busters with Chris Kresser!
Chris Kresser: Yeah, so keep eating that fish. It’s good for you, and it’s going to improve your health, not harm it.
Steve Wright: It’s always about the scale, isn’t it? It’s always about in relation to other things.
Chris Kresser: That’s right. Even water can be a toxin at a high enough dose.
Steve Wright: So, stop drinking water, everyone. Just kidding. OK, Chris, we really appreciate that AP bulletin you put out there. It was very well done. I had seen a lot of the fear mongering as well. Hopefully they do get those reactors under control out there and can hopefully avert any more problems.
The truth about “eating too much meat”
Let’s roll on to some Q&A. This first question, I think, a lot of listeners are going to identify with, and I thought it was really well put. This comes from Lauren, and, Chris, she wants to know: “Are there any concerns about excess meat consumption for those of us on an autoimmune diet or a similar plan who can’t have eggs or nuts for protein? My main protein sources are grass-fed beef, salmon, and sardines with chicken occasionally. I’m not sure what percentage of my diet comes from meat. Are there potentially detrimental effects from this long-term high consumption of meat, and if so, is there anything I can do to mitigate these effects?”
Chris Kresser: I’ve never seen any evidence that suggests that there would be any detrimental effect. All of the concern about eating too much meat was primarily based on fear of saturated fat, and we now know that saturated fat isn’t a major contributor to cardiovascular disease or metabolic disease, and I haven’t really seen any evidence that it’s a major contributor to any disease. And you’re eating beef, but you’re also eating sardines and chicken, other types of meat, so you’re getting different types of fatty acids there. Meat is very nutrient dense. It is, in fact, more nutrient dense than a lot of vegetables and fruits, especially when you’re considering the nutrients that are known to be essential for human health and not phytonutrients and antioxidants and things that are certainly beneficial, but not necessarily essential. So, no, I don’t really see any problem with that. The only thing that comes to mind is that some people have a genetic predisposition to accumulate excess iron, and if that’s the case, eating a lot of red meat could be problematic because it could increase iron levels, but that’s easily tested for just by getting your iron levels tests once a year or something like that, an iron panel and ferritin. And that doesn’t affect everybody. Most people just excrete any excess iron that they take in from food, so it’s not a concern that everybody needs to pay attention to. It’s only for a small segment of the population.
Steve Wright: Chris, I’m concerned Lauren didn’t mention bacon.
Chris Kresser: She didn’t mention bacon, yeah. You know, it’s not for everyone. Amazing, huh?
Steve Wright: I think there might be an underlying question here, Chris. When you’re eating a high-meat diet like this, could there be a protein consumption problem?
Chris Kresser: It’s really unusual for anyone to eat more protein than is healthy for them without trying hard. Humans can generally deal with up to 30% to 35% of total calories from protein without experiencing any chronic long-term health problems. Once you exceed 35% of total calories, you start to develop the possibility of ammonia toxicity or ammonia overload, urea ammonia issues, but that’s really, really rare and it usually happens with bodybuilders or people who are taking lots of lots of protein powder and eating super-high protein diets to try to put on muscle mass or something like that. We have a system in our brain that kind of regulates protein intake, and when we need more, we crave more protein, and when we need less, we’re averse to it. If you yourself have ever been pregnant, women listening to this show, or you know someone that has, you probably either yourself or know someone who experienced extreme protein aversion during some point during pregnancy. That’s not an unusual symptom, and there’s some evolutionary reasoning behind that, and women generally crave less protein during pregnancy and can sometimes even feel nauseous when they think about protein or high protein foods during pregnancy. That’s not always the case, but it does happen. So, generally the brain will regulate it well, and even if you’re eating meat at every meal, it’s unlikely that you’re going to exceed 35% of total calories from protein.
Naturally healing cavities
Steve Wright: Awesome. Let’s move on to the next question, Chris. This one comes from Josie. She’s seen several claims that eating a diet similar to yours, Chris, plus taking grass-fed butter oil and fermented cod liver oil heals cavities. Is this a fact or fiction? And this continues our myth-busters episode.
Chris Kresser: I haven’t looked into the evidence on this, like in the scientific literature, but certainly anecdotal evidence supports the idea that proper diet can help remineralize teeth. There’s a book called Cure Tooth Decay by Ramiel Nagel, and he talks about using a nutrient-dense diet and superfoods like cod liver oil, raw milk or cheese, raw dairy, bone broth, and maybe grass-fed bone marrow, either raw or cooked, to remineralize teeth and prevent the progression of and, in some cases, even reverse cavities. I know a lot of people and patients who’ve had issues with dental health and switched to a nutrient-dense diet and seen really big changes, so I think it’s possible, based on anecdotal experience.
There are also special probiotics that you can use for dental health. Streptococcus salivarius K12 and M18 are two special species that have been shown in clinical studies to have benefits for dental health, and they work by attacking some of the bacteria and plaque, and also they break up the biofilm which plaque is formed from, and that can be really difficult to do otherwise. Generally these probiotics, you get them and you put them in water, and then you swish them around in your mouth on a daily basis, and that can lead to significant benefits as well.
And then some people use xylitol chewing gum for reducing biofilm and cavities, but I’ve read a couple reviews that suggest that while it’s true that sugarless chewing gum has been shown to reduce cavities, it’s not the xylitol in the gum that’s doing it. They did a study where they gave people xylitol lozenges rather than chewing gum and there was no reaction, no reduction in cavities. The author speculated that it was maybe active chewing which increased the salivary flow that led to the benefit of reduced cavities rather than the xylitol itself, but nevertheless, some sugarless gum has been shown to help in that way. You have to be careful with the sugarless gums, though, because, of course, a lot of them contain artificial sweeteners, and xylitol is a FODMAP and can be difficult for people with digestive issues. And then some of the other artificial sweeteners have been shown potentially to have adverse health effects. The research is a little mixed on that, and I’m not ready to make a definitive statement, but there are some studies that suggest that they may be harmful, so I think the better choice is to do the oral/dental probiotics and then the nutrient-dense superfoods, the fermented cod liver oil/butter oil blend has vitamin A, vitamin D, vitamin K2. All the fat-soluble vitamins are especially helpful for dental health. Then you have the grass-fed dairy, also a great source of K2 and vitamin A. You have bone broth soup, which will have minerals, calcium, glycine, which is helpful for tissue rebuilding, and then the bone marrow and organ meats are also incredibly nutrient dense as well. So, if you do all that and the dental probiotics, I think that’s a great place to start.
Steve Wright: Yeah, and I think we couldn’t mention this without saying that if you haven’t read Weston A. Price’s book, you should probably just read that if you’re interested in this topic.
Chris Kresser: Absolutely. And that’s what Ramiel Nagel’s book is based on. He’s a member or has been involved in the Weston A. Price Foundation, and he’s known in that community, and that’s what his approach is based on, although I think he’s more along the lines of paleo plus raw dairy because he’s not a fan of grains for people who have dental issues, grains or legumes.
Steve Wright: Hmm, interesting. I’m going to have to get that book.
Hepatitis C and Liver Disease
OK, let’s roll on to the next question, Chris. This comes from Anonymous. First off, they have hepatitis C, and they’re mostly asymptomatic with the exception of debilitating fatigue. They follow a super-strict paleo diet and have never drank alcohol… well, at least lately. The last drink that this person had was on December 31, 1999. They’re now 46 years old and have had the virus for around 25 years. Getting to the question, they would like to know, should they get a liver biopsy to determine if they have cirrhosis, so liver cirrhosis? Their mom is adamant that sticking a needle into the liver is a bad idea and that once you start cutting and poking and doing these types of invasive things that it might lead to cancer. It’s a wacky theory, but she’s adamant about this. So, what this woman is looking into is a doctor named Dr. Sylvestre in Oakland who treats hepatitis C with ribavirin and interferon. She treats everyone regardless of whether they have healthcare. She has a remarkable cure rate unless cirrhosis is present, but even then, she still will recommend treatment. She is somewhat of a hepatitis C guru. But this person has a question, Chris. She’s terrified of what these drugs will do to her gut, brain, and bones. She would like to know what you would do if you were her.
Chris Kresser: OK, so let’s break this up a little bit. The first question was about liver biopsy and whether that’s a useful test. It is useful in the sense that it can provide useful information, but her mom is correct in that it’s invasive and potentially dangerous. There were adverse effects that can happen with liver biopsy, and actually many doctors are even hesitant to recommend it at this point because of that. Sticking a large needle into your liver is definitely not risk free. Luckily, there is a test called FibroSURE, which is a combination of six serum tests, six blood tests, and it generates a score that is correlated with the degree of liver damage in people with a variety of liver diseases, and it actually has been clinically validated to have the same prognostic value as a liver biopsy with a tiny fraction of the risk, and the risk is only the risk that you would be exposed to by getting blood drawn, which is very, very small now. The six tests are A2-macroglobulin, haptoglobin, apolipoprotein A1, bilirubin, GGT, and ALT, and with the exception of A2-macroglobulin and apolipoprotein A1, they’re fairly commonly available tests, but when they put that together into a certain algorithm or score, that score is as good of a marker for liver issues as the liver biopsy. And there’s a hep C FibroSURE that you can take that I would definitely recommend instead of a biopsy.
The other test that’s useful for tracking hep C over time is the reverse transcription polymerase chain reaction test, or HCV RT-PCR, and that’s used to monitor the status of hep C over time. It basically tells you the viral load and the amount of disease activity that you’re experiencing, and you can use it as a barometer for how treatment is progressing, and that should go down over time if the treatment is working, so you could run it, like, every six months as a way of gauging the success of the treatment. So, those are things to definitely talk to your doctor about.
In terms of treating hep C, it’s, of course, a virus, and like all viral infections, often the best approach is to strengthen your own innate immunity as much as possible and then to use additional things that are specifically antiviral on top of that. We’ve on several shows, I think, talked about basic nutrients for immune support. That would be vitamin C, glutathione – I like the liposomal forms of both of those. Selenium and zinc. There are some botanicals that have very impressive immune-boosting ability. One combination that I like is equal parts of astragalus, Cordyceps, and rhodiola. You just take 30 or 40 drops of that or maybe twice that dose three times a day. And then you have antiviral nutrients, like Lauricidin, which is an extract of lauric acid, monolaurin. That’s antiviral and also has activity against biofilm and gram-negative bacteria and fungi. Apolactoferrin is antiviral. EDTA, which is in InterFase Plus; it has activity against biofilm, but also it’s antiviral. And then you have some antiviral herbs, like Chinese skullcap, elder, ginger. Licorice, a lot of people don’t know, is strongly antiviral. Lomatium, which is biscuitroot, another name for it, and rhodiola also has antiviral activity.
So, there are a lot of different alternative approaches to treating viral infections, including hep C. I’m not familiar with that particular physician and her work, so I can’t really comment on that, but there are a lot of people around the Bay Area, if that’s where you are, herbalists and alternative practitioners that specialize in these kinds of treatments if you don’t want to go the drug route, but that’s, of course, something you’d need to discuss with your doctor.
What to do about esophagitis and GERD
Steve Wright: OK, let’s roll on to the next question. This one comes from Heather, Chris. She’d like to thank you for all the wonderful articles that you’ve written on heartburn and GERD. However, she did not see any mention of how to heal existing esophagitis. She has a “15-year-old son who just recently had an endoscopy, and his GI doctor showed me the photos of his very inflamed tissue. Apparently the biopsy came back negative for H. pylori, and the GI doc wants to put him on Prilosec. I’m planning on finding someone to do a Heidelberg capsule test for him just so we can figure out what we’re truly dealing with, but I’m concerned about getting his existing damage healed. Could you comment and provide any suggestions about this?”
Chris Kresser: Yeah. I mean, the best way to stop the tissue damage and reverse it is to stop the GERD from happening, and the body actually has a remarkable ability to heal tissue in many cases, so if you stop the insult from continuing to occur, then especially for a 15-year-old, their regenerative capacity is often quite a bit stronger than someone who’s a lot older, and it will often heal on its own. But there are a few things you can do to help things along. Marshmallow, slippery elm, and deglycyrrhizinated licorice – that’s DGL – they’re all botanical plant substances that are mucilaginous. They have a really soothing and healing effect on tissue, mucosal tissue in particular. Manuka honey – or any honey, actually – is one of the best wound-healing substances there is. It’s even used in a lot of hospitals now. There’s a lot of scientific literature on this. A lot of people are surprised and they kind of consider it a folk remedy, but if you go on PubMed and do some research, you’ll see there’s a lot of studies on it, and there’s also an extremely long tradition in all different kinds of cultural traditional medicines of using honey for wound healing. Manuka honey from New Zealand, I think, seems to work best, but other raw forms of honey will do it. Zinc carnosine and MSM are both mucosal protective and anti-ulcerative. And then glycine, which is an amino acid found in cartilaginous types of meat, tougher cuts like oxtail, shanks, brisket, chuck roast, and then drinking one to two cups of bone broth a day made from chicken – make sure to include the heads and feet – and femur bones and marrow bones from beef. These are all things that can really help with rebuilding the tissue layer in the esophagus. And one product that has a number of these things in it is GastroMend from Designs for Health. That’s something I use. So, you could do the GastroMend plus some honey plus glycine-rich foods, and I think that would be a great start.
Is resistant starch useful?
Steve Wright: Yeah, sounds like a great protocol. OK, let’s roll on to the next question. This question comes from Joss. “Chris, what’s your take on resistant starch? Do you think it can be useful as a prebiotic? How about other uses such as hunger control, etc.?”
Chris Kresser: Yeah, I am pretty interested in resistant starch. I’ve been studying it quite a bit lately and using it in my practice. It’s a type of insoluble fiber that’s fermentable by gut bacteria. There are several different types of fiber. The two main categorizations are soluble and insoluble. Soluble fiber is fermentable by gut bacteria, and I consider it to be more beneficial for that reason. Insoluble generally isn’t, but resistant starch is a type of insoluble fiber that is fermentable, so it can be used as a prebiotic to increase the levels of beneficial bacteria in the gut, but it’s also – and I would say primarily – being used now for blood sugar management and metabolic issues. It seems to have a pretty significant impact on especially fasting blood sugar. I’ve seen 10-or-15-point drops and heard of even greater reductions in fasting blood sugar just by using resistant starch.
It’s difficult to obtain in food. One way to get it is in potatoes that have been cooked and then cooled for 24 hours. It’s the cooling that actually transforms the starch in potatoes to resistant starch, so cooked potatoes that haven’t been cooled don’t really have any resistant starch or very little, but potatoes that have been cooled for 24 hours do have a significant amount. Another way is eating green plantains. The only way to make green plantains edible without cooking them is dehydrating them into chips. Green bananas have some resistant starch, but I don’t find them to be very appetizing myself, so the way that most people are using resistant starch is by taking potato starch and mixing it with water. The Bob’s Red Mill variety is gluten free, and you can do 2 to 4 tablespoons a day. If you have a really high fasting blood sugar, doing maybe 3 to 4 tablespoons at night before you go to bed mixed with water is one way you can get the benefits of it.
So, yeah, I think it’s promising and it’s cheap. Potato starch is pretty darn cheap. There’s no risk to it really, and I’ve been hearing about some other interesting metabolic effects, like increases in body temperature with people who have thyroid or adrenal issues. Richard over at Free The Animal has been writing a lot about resistant starch, so if you want to learn more about it, you can go check out his blog, FreeTheAnimal.com. It’s not for kids, let’s just say! There is language. Yeah, but if you’re a consenting adult, you can head over there, and there’s some great information on resistant starch.
And be careful with resistant starch if you have SIBO or other gut issues, like IBS, because as a prebiotic, it can cause some pretty profound changes in the gut flora pretty quickly, and that can, in some cases, increase gas and bloating and lead to some digestive difficulty. The best way to mitigate that is just to go slowly. So, instead of starting with 3 tablespoons, start with a teaspoon and see how you tolerate that and go from there.
Treating skin conditions with FMT
Steve Wright: Awesome. Great advice. Let’s roll on to another digestion-related question, Chris. This one comes from Simon. He wants to know about fecal microbiota transplantation, FMT. “This has been gaining a lot of attention lately, and most of it is regarding treating ulcerative colitis or IBS” – and I’ll add in C. difficile. He wants to know specifically is it possible for FMT to be used for treating skin disorders, such as psoriasis?
Chris Kresser: Yeah, so we’ve talked about fecal transplants on the show before, and I’ve written about them on my blog. It’s a very exciting new treatment, and I think it could potentially benefit many different conditions, including skin conditions because of the gut-skin axis, but also depression and other kinds of cognitive behavioral issues, possibly even autism. The gut-brain axis we’ve talked about a lot. The fact is there isn’t really much in the body that’s not affected by gut and gut health, and every month there is an increasing number of studies published that directly link gut health to things that aren’t apparently related to the gut, like Parkinson’s disease, Alzheimer’s, like I said, depression and autism, all different types of autoimmune diseases, skin diseases. It’s really difficult to find conditions that aren’t in some way affected by the gut microbiota now, and I think our awareness of that is only going to increase. So, potentially FMT could affect a very broad range of medical conditions.
The problem is it’s inaccessible to most people. In fact, it looked like it was going to become more accessible and that people were starting to use it and study it for a lot of other conditions, and it is still being studied for other conditions in research setting, but the FDA just come out with some rules that suggest that it can only legally be used for antibiotic-resistant C. difficile, which is a gut infection that can be lethal, especially if it’s antibiotic resistant. So, the only case in which a doctor is legally allowed to perform it is with someone who has antibiotic-resistant C. diff, and in that case, it can certainly be a life-saving treatment almost overnight. This means that we’re starting to see an underground where people are performing these procedures at home because they read about it and they’re really interested and they want to do it themselves and try to get some of the benefits. And I completely understand that, and in some way, I’m in support of the idea behind it and the treatment itself, but I do want to caution people that it is not a risk-free treatment, and it is potentially dangerous if it’s not done correctly, and it’s potentially dangerous if the donor isn’t screened adequately, which, I think, almost always is the case when people are doing it at home.
A lot of diseases can be transmitted via the stool, and there are certain bacteria, parasites, etc., that might be in your donor that aren’t causing problems for your donor because their overall microbiota is strong enough that they keep those things in check, but when it’s transferred into someone who is immunocompromised and has a different baseline microbiota, then those organisms could become problematic. And I’ve also heard and read about some reports of changes in mood and personality after receiving gut microbiota transplant, and if you think about it and we’ve talked a lot about how the gut microbiota affect behavior and the brain, getting someone else’s gut microbiota in your gut could potentially affect your behavior and your brain and your cognition.
So, there’s a lot more to it, I think, than some people realize in terms of what can go wrong, and while I’m extremely enthusiastic about its potential and I’ve seen it really work miracles in people, I’m a little bit more cautious than maybe some of my colleagues and a lot of people in the general public because I’m just a little bit more circumspect about it because of what can possibly go wrong. And I know myself as a clinician, back before these FDA regulations when I was looking into it when people would be curious about it and wanted to find a donor and were going to be working with another doctor, perhaps, to find a donor, I would help them to screen their donors, and I’m telling you that probably 8 out of 10 times the donor would fail some aspect of the screening process. I was using labs for screening stool that are more sensitive and specific than the typical stool tests that you get at, like, Quest or LabCorp, and so I probably was picking up on more stuff than someone who went through a more general screening process. And then I was also excluding people if they had autoimmune disease, which I think should absolutely be done because we know that a lot of people with autoimmune disease have gut issues and vice versa. So, my criteria were strict, but they weren’t any more strict than the new – You know, I just read a paper about the new criteria for donors, and my criteria was right in line with that, and it was really hard to find qualified donors.
So, my fear is that people will do this at home, they won’t adequately test the donor, they’re just kind of desperate to get well, which I completely understand, but then they transfer stool from a donor who’s not suitable for whatever reason, and even though that person’s not sick, the recipient gets sick or more sick because their own microbiota is not compatible with something that came into them from the donor. As I’ve said before, I’m excited about it, I think it has great potential, but I think it also deserves caution, and if you’re thinking about doing it at home, please get proper supervision and do it with someone who knows how to screen a donor properly, etc. That person will be doing it illegally, so I’m not advocating this, but I’m saying if you’re the kind of person who’s just going to do it anyway, really, please do it with supervision.
Steve Wright: Yeah, I think that’s beautifully put, Chris, and I think everyone should definitely remember that the ways in which your gut microbiota, everywhere from your mouth all the way to the anus, how it works within your body is still misunderstood. I mean, we don’t know how many ways it affects you, and so these changes in behavior and even what can happen from just wiping out that gut bacteria from a colonoscopy prep and/or an antibiotic route changes that forever, so when you’re thinking about overhauling everything with some sort of treatment like this, as Chris said, follow his idea.
Chris Kresser: Yeah, you alluded to this, Steve, but the Human Microbiome Project has told us that every person’s gut flora is unique, like a snowflake or a fingerprint. And so, the consequences of transferring someone else’s microbiome into you are unknown. I mean, certainly there’s a lot of evidence that suggests it can be extremely beneficial, so I’m not diminishing that evidence. And if it’s a life-threatening situation where someone has C. diff and they’re at death’s door, then the risk is deemed to be less than the potential benefit, which is staying alive, right? I mean, there’s no question in that situation. In fact, the paper that I read was suggesting that in those cases you don’t even need to screen the donor because if you have a healthy donor that’s available, the benefit of keeping that person alive is far greater than the potential risk of something else being introduced in that circumstance, especially if it’s a close family member. So, yes, very promising, and I completely understand. I mean, the people who are considering this procedure are generally people who have tried a lot of other stuff and haven’t had success, and it’s so alluring to think that you could do this one procedure and then literally overnight have a pretty profound change in your health, and that sometimes does happen, so it’s extremely appealing from that perspective, but I just want people to consider some of the potential risks that haven’t been articulated or talked about much in the alternative medical community regarding this procedure.
Steve Wright: Yeah, and I don’t want people to get me wrong. I think it’s an amazing procedure. I’ve talked with many people who have had it and seen the same kind of benefits that Chris just talked about, but as Chris said, I think not enough people actually talk about the full range and scale of effects that treatments can have, whether they be alternative or conventional, so it was a great discussion.
Chris Kresser: Exactly. All right, well, I hope you enjoyed the show. I hope it was worth the wait, and we’ll have another one for you soon. Thanks, everyone, for your continued support. I’m really excited about the book. It’s now been copyedited and I’m about to get the final pages proofed – I think they call them pages, where I make any small, last-minute changes. And then in mid-October, that’s it. It goes into the print production process, and we’ll start doing a lot of cool stuff.
Steve Wright: That’s when you go to the Bahamas, right?
Chris Kresser: Yeah! Not exactly! That’s when a lot of other work starts related to the book, but you’ll be hearing more about it in the months to come. I’m really excited about it. I actually was in New York last week doing a media lunch that my publisher put together with some people from the media, and I got a chance to see the book bound in pre-pre-production form in a softcover form, but it was pretty exciting to see it in its bound form for the first time.
Steve Wright: Well, I’m pretty excited to see it. I know you’re working hard, Chris, and we’re going to continue to try to get these podcasts out as you have time. So, thanks, Chris, for taking time today. Thanks, everyone, for listening to this podcast. Just so you know, you can always submit your questions for these Q&A episodes at ChrisKresser.com using the podcast submission link. And Chris and I would really appreciate it if you enjoy these episodes to go over to iTunes, leave us a review, and let us know what we’re doing well and what we could do better.
Chris Kresser: Thank you, Steve, and see you all next time.

 About Laura: Laura uses her knowledge of traditional and biologically appropriate diets to improve her clients’ health. Growing up with a family that practices Weston A. Price principles of nutrition, she understands the foods and cooking practices that make up a nutrient dense diet.
With her strong educational background in biochemistry, clinical nutrition, and research translation, she blends current scientific evidence with traditional food practices to help her clients determine their ideal diet.
You can find her at
About Laura: Laura uses her knowledge of traditional and biologically appropriate diets to improve her clients’ health. Growing up with a family that practices Weston A. Price principles of nutrition, she understands the foods and cooking practices that make up a nutrient dense diet.
With her strong educational background in biochemistry, clinical nutrition, and research translation, she blends current scientific evidence with traditional food practices to help her clients determine their ideal diet.
You can find her at 

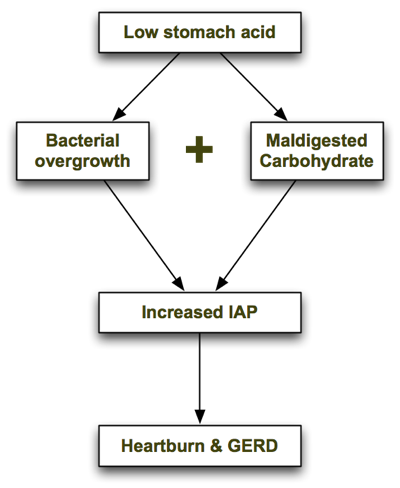 Let's look at each step in turn.
Low stomach acid causes bacterial overgrowth
As I will explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can't survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The
Let's look at each step in turn.
Low stomach acid causes bacterial overgrowth
As I will explain in the next article, one of the chief roles of stomach acid is to inhibit bacterial overgrowth. At a pH of 3 or less (the normal pH of the stomach), most bacteria can't survive for more than 15 minutes. But when stomach acid is insufficient and the pH of the stomach rises above 5, bacteria begin to thrive. The 









